delta dental application form
Relocated out of Massachusetts Have other Dental Plan Other Non-payment Deceased 13. PDF forms may be downloaded.
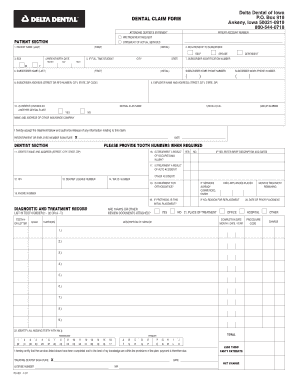
Delta Dental Of Ia Claim Form Sioux City Community School District Fill Out And Sign Printable Pdf Template Signnow
Join our dentist network.
. This will allow Delta Dental of Washington to release relevant information to the chosen party. Direct Debit Authorization ACH Form. Delta Dental PPO participation packet request.
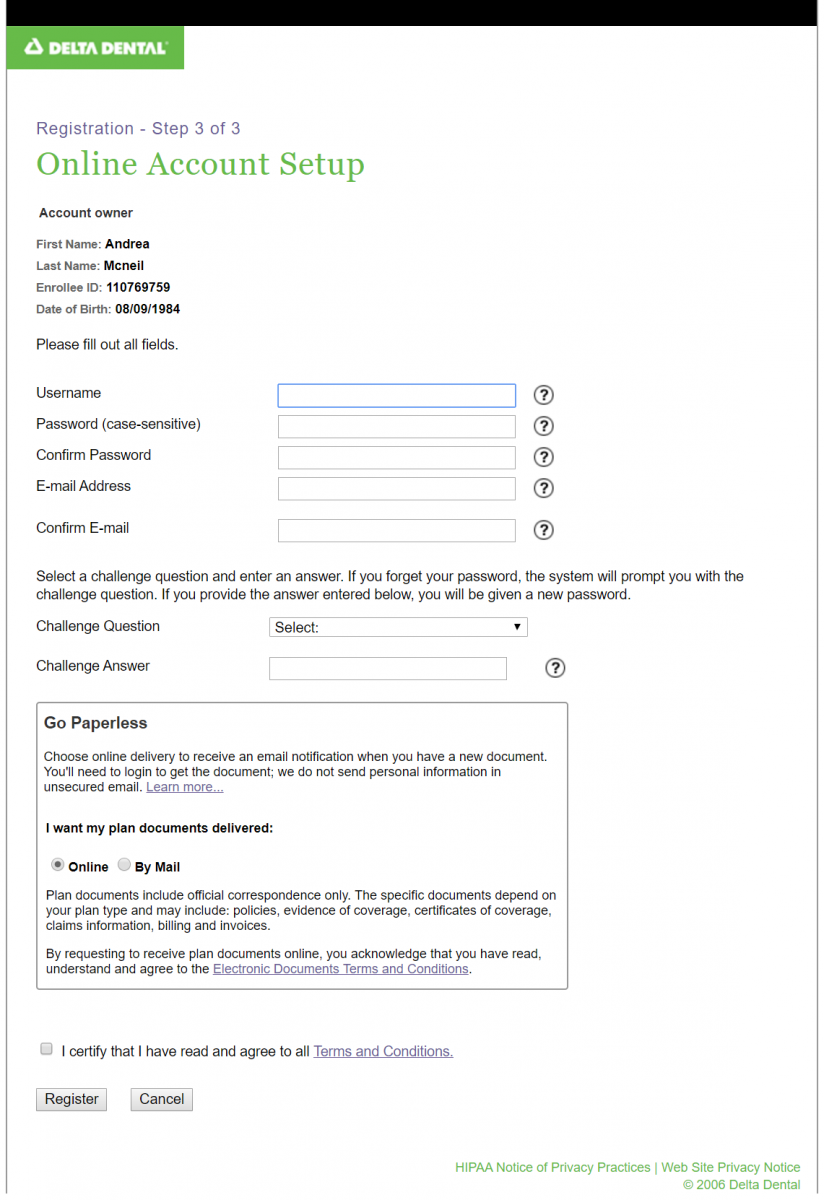
To access a dental claim form enrollees can log into Member Portal. Authorization Agreement for Automatic Payments. More Americans choose Delta Dental than any other dental insurance provider.
ASO contract addendum for HIPAA privacy and security. Find the forms and resources to assist you in administering Delta Dental of Oklahoma benefit products and services. Thats why most dentists choose to work with Delta Dental to protect their patients.
Customer Service hours will be 945 AM to 445 PM ET. Healthy Smile Healthy You. Delta Dental HIPAA Form 14a Risk Groups.
Please complete all sections of. Delta Dental HIPAA Form 14b ASO Groups. MNND Eligibility EnrollmentUpdate Form.
Friday November 18 2022. Dentist Administrative Forms and Resources. Issued by Delta Dental you must sign and return this form with your application.
Find the useful forms to assist you with selling and administering Delta Dental of Oklahoma products and services. FIRST NAME REASON FOR SUBMISSION 14. Use this form to view overage dependents information or if youre having custody issues.
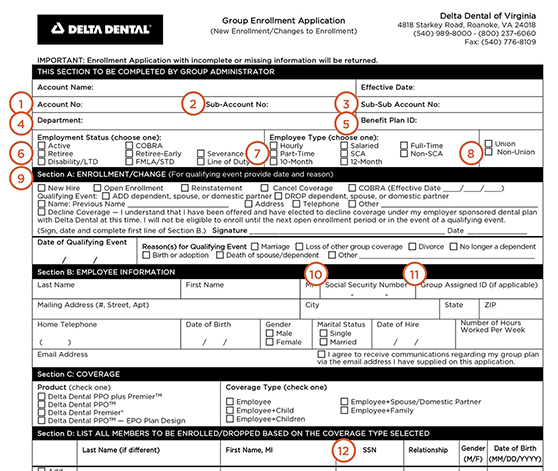
For your own information and protection certain facts should be pointed out to you which could affect your. MN Membership Enrollment Form Spanish Small Group Pooled MN ND Enrollment Form for. Enrollment application change of information form Dual Dental To expedite your application please print legibly in black or blue ink and return as instructed.
To view benefit information and claim status. Easily download and submit the form or application that relates to your needs. Locum tenens provider form.
They can also call Customer Service at 877 395-9420 or send an email to. We apologize for any inconvenience this may cause. General Change Form for Groups.
Dental screening by a PCP includes monitoring of tooth eruption occlusion pattern presence of caries oral infection and referral to a primary care dentist PCD for a full exam and treatment. LAST NAME if different from subscriber 15. Request for Proposal Request for Proposal Information Form Business.
Dental Illinois Institute Of Technology

Dental Insurance Forms Delta Dental Of Washington
Enrollment
Dental Insurance
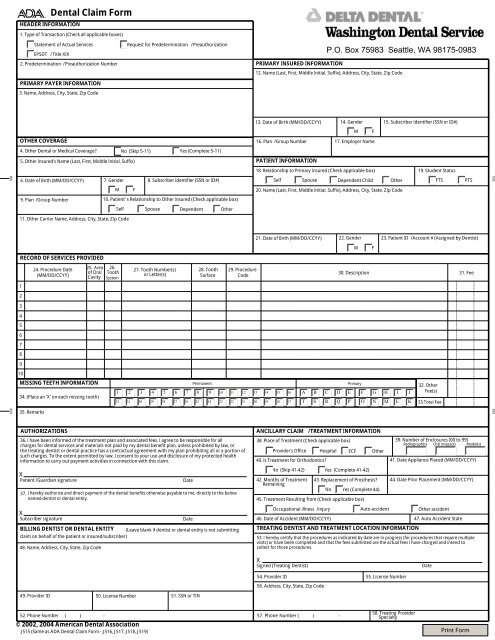
Delta Dental Claim Form Washington Dental Service

Member Forms And Downloads Minnesota
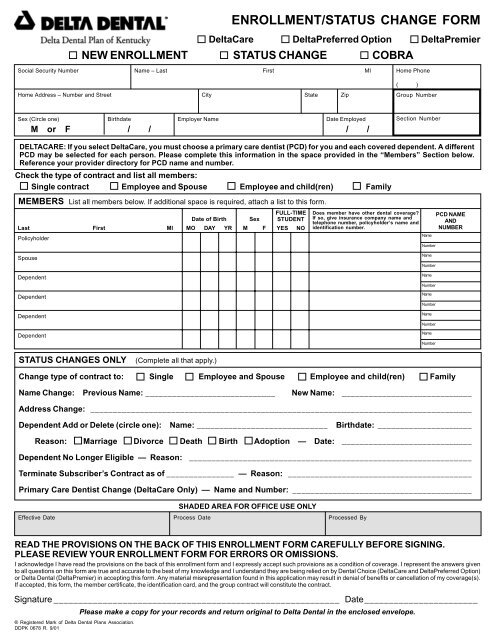
Delta Dental Enrollment Form
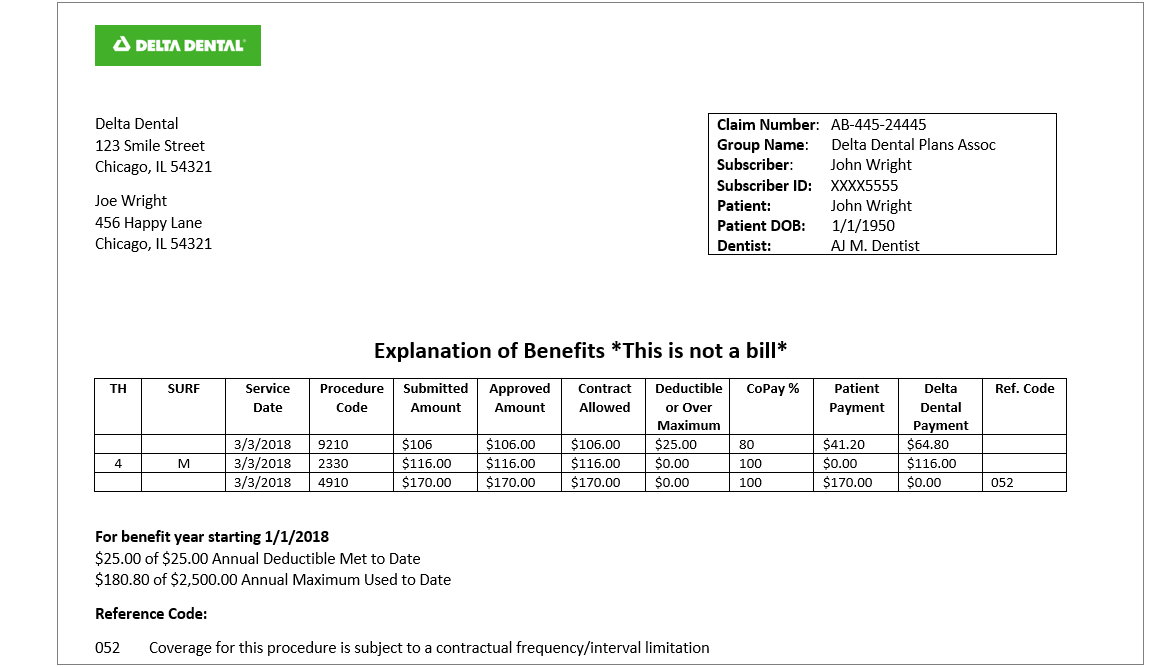
All About Dental Explanation Of Benefits Eob Delta Dental
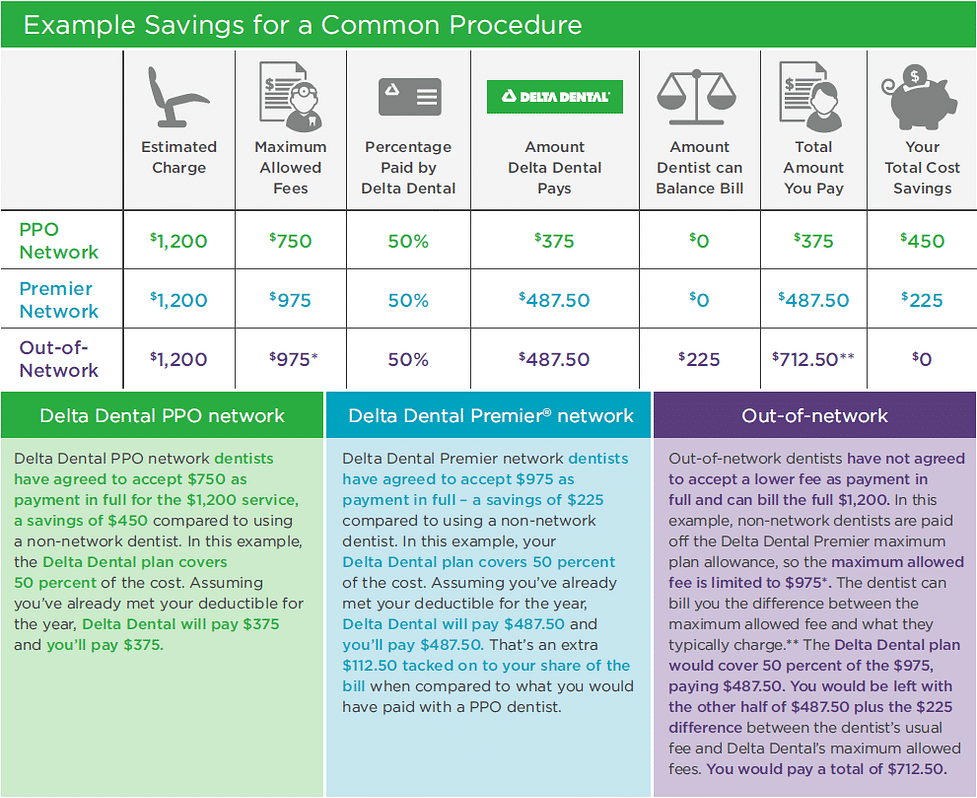
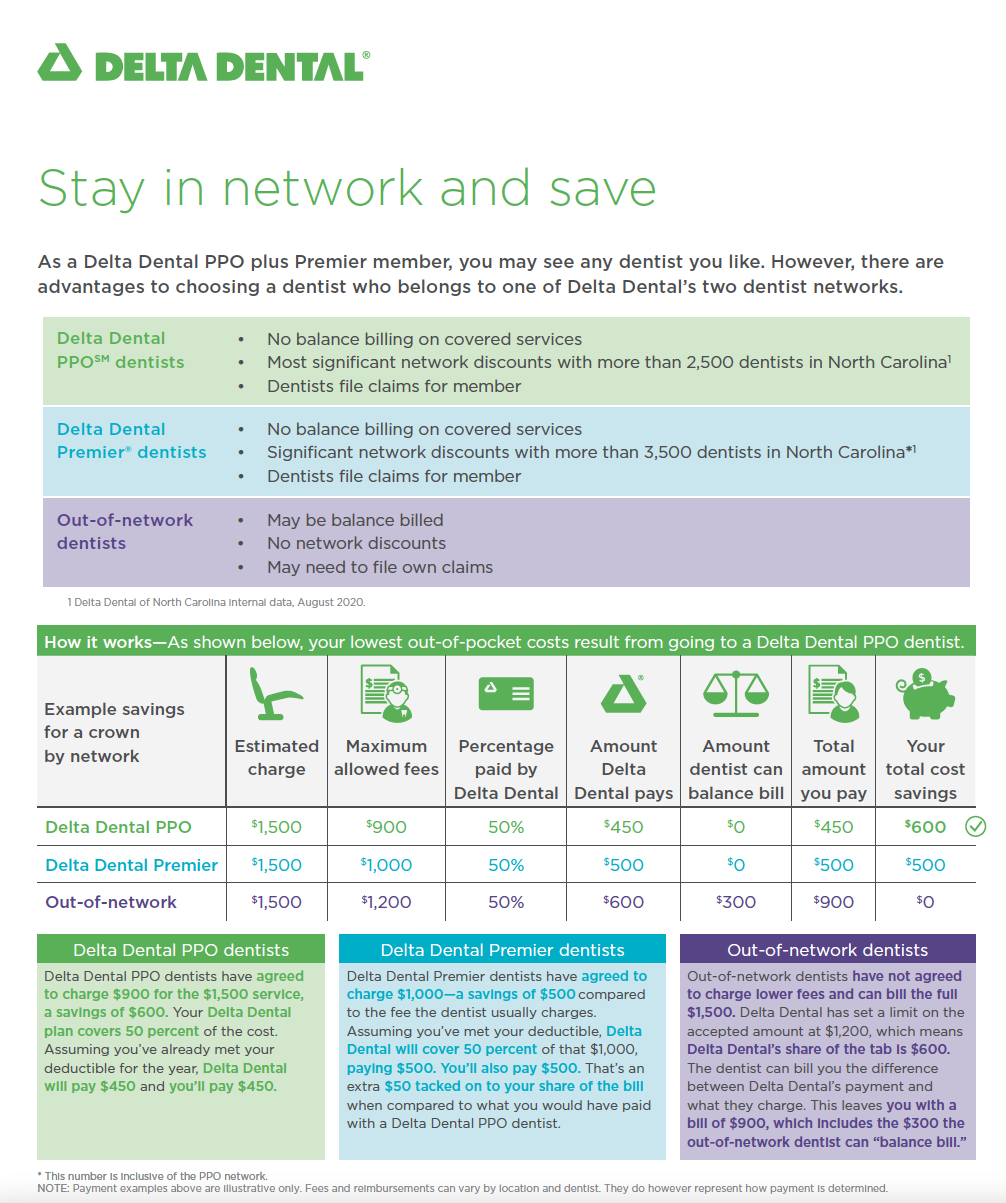
Ppo Vs Premier Dental Coverage Delta Dental Of Illinois
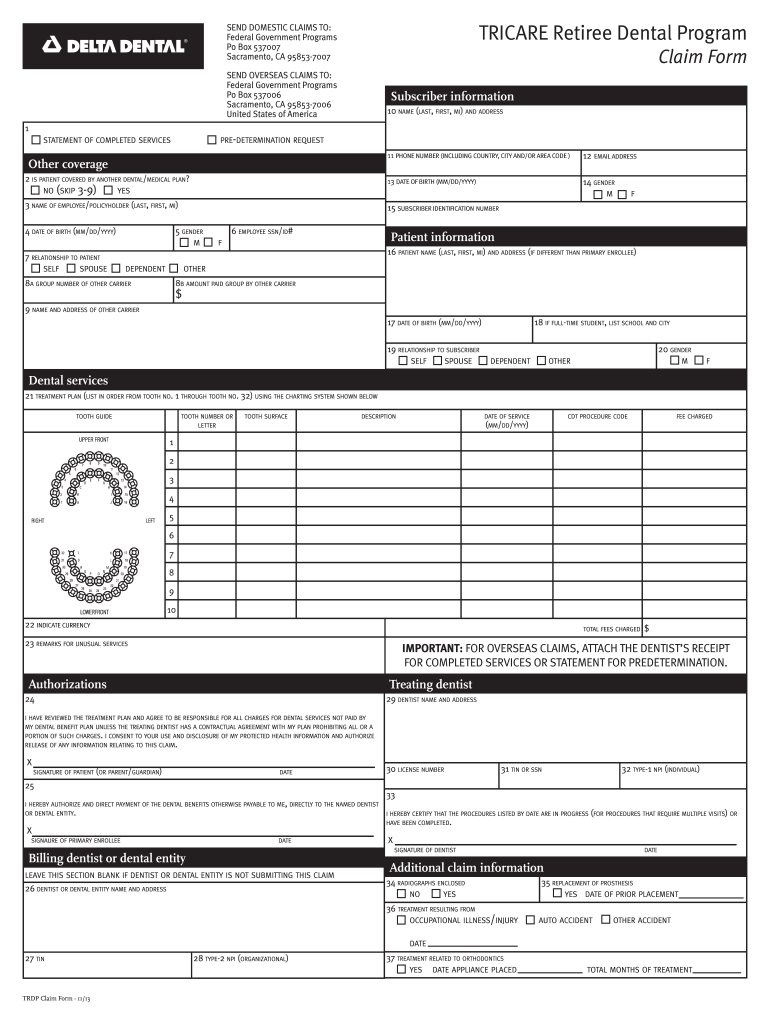
Tricare Dental Claim Form Fill Out Sign Online Dochub
Delta Dental Claim Form Fill Out And Sign Printable Pdf Template Signnow
Fillable Online Deltacare Usa Claim Form Delta Dental Insurance Fax Email Print Pdffiller
Delta Dental Group Spanish Healthcare Reform Certified Hcr Plans Membership Enrollment Form Fill And Sign Printable Template Online
Dental State Employees Association Of North Carolina

Can My Dentist Charge Me More Than My Dental Benefit Plan Allows

Delta Dental Enrollment Form
Fillable Online Delta Dental Fillable Enrollment Form Fax Email Print Pdffiller
![]()
Delta Dental For Dentists Delta Dental
Dental Insurance